Locked In
 This is the story of an unfortunate gentleman whom I admitted a few weeks ago. He presented initially to an outside hospital with nausea, vomiting and vertigo, a rather mundane complaint in most EDs across the world but this particular individual understandably excited fear and trepidation amongst the ER staff because of a "ginormous" dilated basilar artery with a distal saccular aneurysm that prompted the feared phrase: "needs neurosurgical evaluation" which often translates to "admit to neurology."
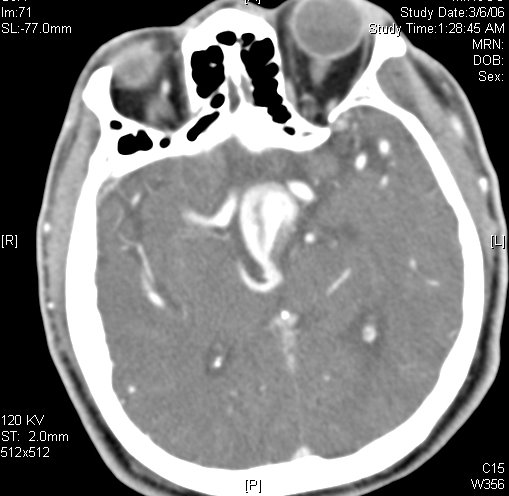
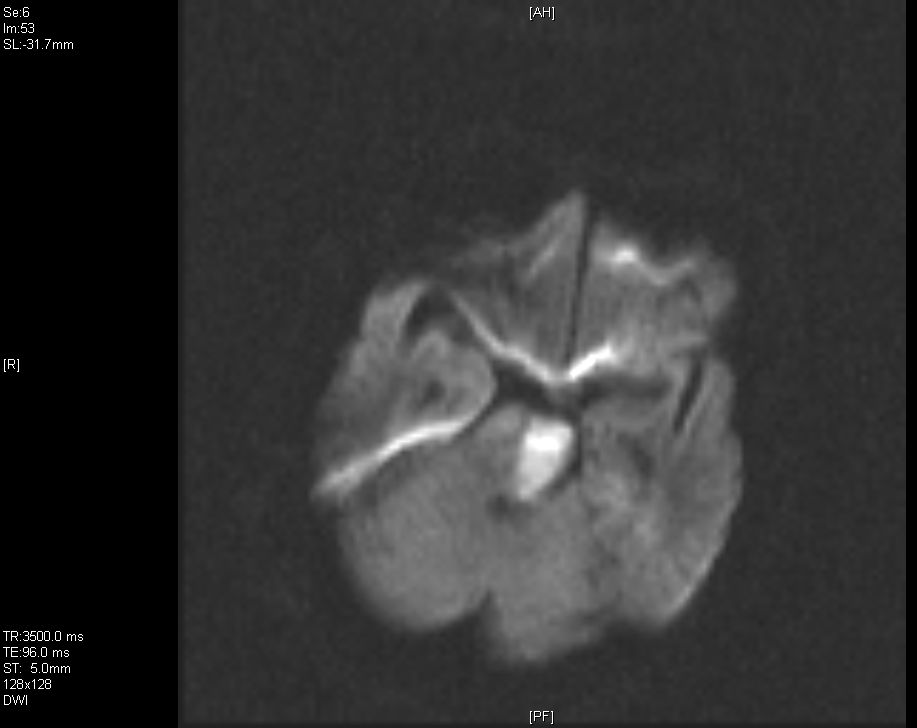
This is the story of an unfortunate gentleman whom I admitted a few weeks ago. He presented initially to an outside hospital with nausea, vomiting and vertigo, a rather mundane complaint in most EDs across the world but this particular individual understandably excited fear and trepidation amongst the ER staff because of a "ginormous" dilated basilar artery with a distal saccular aneurysm that prompted the feared phrase: "needs neurosurgical evaluation" which often translates to "admit to neurology."He was therefore summarily transferred to our hospital for neurosurgical evaluation. It was discovered on CT angiography (see right; the next inferior image is taken from a december catheter angiogram at which time an unsuccessful attempt was made to coil the aneurysm) that though large and frightening said aneurysm was in fact intact, ie had not ruptured. To complicate things however on the ride over from the outlying hospital the patient acutely developed right-sided weakness and a profound dysarthria without aphasia, raising our concern for a brainstem event. Our fears were confirmed on subsequent diffusion weighted MRI image which showed a complete left hemipontine acute infarction (third image) likely due to occlusion of a pontine penetrator from the severely diseased basilar.

The patient remained stable over the following week but then on the weekend in the setting of a relative hypotensive episode developed left sided weakness. Shortly thereafter he was intubated for respiratory distress, likely due to floppy airway from decreased bulbar tone and apparently responded to this extremely noxious procedure with mere contraction of his bilateral masseters, ie he bit down. This raised our suspicion and concern for one of the most feared diagnoses in all of neurology: "the locked-in syndrome."
The so-called "locked in syndrome" is essentially a fate worse than death. It is described in Blumenfeld's Neuroanatomy text as consisting of a loss of motor function via interruption of the corticospinal and corticobulbar "long tracts" in the ventral pons. Despite this near total paresis both sensation and cognition are entirely intact. It can be the result of pontine stroke, hemorrhage, tumor, encephalitis, multiple sclerosis, or central pontine myelinolysis as a result of too zealous correction of hyponatremia. Movement is totally impossible as there is no efferent input from the cortex to initiate movement but the torturous component comes from the fact that reticular activating system ie consciousness and ascending afferent sensory pathways are intact. In other words you can still have an itch and know that you have an itch but can't do a damn thing about it. At times, a locked in state can be confused with coma given the total lack of movement but the locked in individual is in everyway like you and me sans movement. Because vertical eye movements and eyelid deviation are controlled by the tegmentum of the rostral midbrain which lies cranial to the pons these latter movements can be preserved and sometimes be the only means by which the locked-in person can communicate with the outside world, sometimes using computer interfaces (below is a DW image taken after the second decompensation showing bilateral pontine restricted diffusion, ie a bilateral pontine stroke).
 I am told there is an excellent if tragic book actually written by someone who was locked in, communicating in code with blinking movements of his left eye called The Diving Bell and the Butterfly : A Memoir of Life in Death by the French editor of Elle magazine Jean-Dominique Bauby. I cannot yet reccomend it personally but it it is praised by trustworthy sources. And, apparently, according to the Internet Movie Database it has been fast-tracked by one of the movie studios for production into a film starring (I shit you not) Johnny Depp.
I am told there is an excellent if tragic book actually written by someone who was locked in, communicating in code with blinking movements of his left eye called The Diving Bell and the Butterfly : A Memoir of Life in Death by the French editor of Elle magazine Jean-Dominique Bauby. I cannot yet reccomend it personally but it it is praised by trustworthy sources. And, apparently, according to the Internet Movie Database it has been fast-tracked by one of the movie studios for production into a film starring (I shit you not) Johnny Depp.Locked-in syndrome raises numerous philosophical issues regarding consciousness and its definition as well as ethical patient care. There are attempts afoot to develop effective brain computer interfaces to allow those who are locked in to effectively interact via their world via prosthetic devices. And at times people do recover from this horrific state. Our patient, however, was not one of the lucky ones. He succumbed to likely respiratory failure when his family humanely decided to withdraw support.
posted by Der Leierman @ 12:06 PM
0 comments
![]()
![]()

0 Comments:
Post a Comment
<< Home